Of all the peripheral nerve injuries that occur in the operating room, peroneal nerve damage is among the most preventable and among the most commonly overlooked. In lithotomy procedures, where the patient’s legs are elevated and supported in stirrups for extended periods, the common peroneal nerve is under consistent mechanical risk. The wrong support setup, or no dedicated support at all, can leave this nerve compressed against the fibular head throughout the entire procedure.
The consequences can show up days after surgery: foot drop, numbness along the outer leg and foot, or weakness in ankle movement. For patients already recovering from a procedure, these complications add real clinical burden and often require extended rehabilitation.
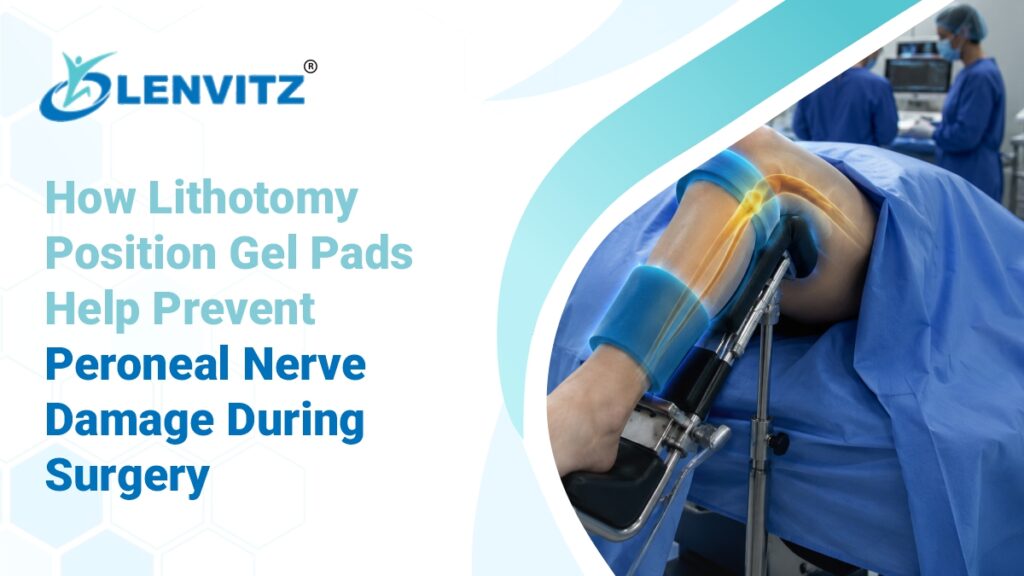
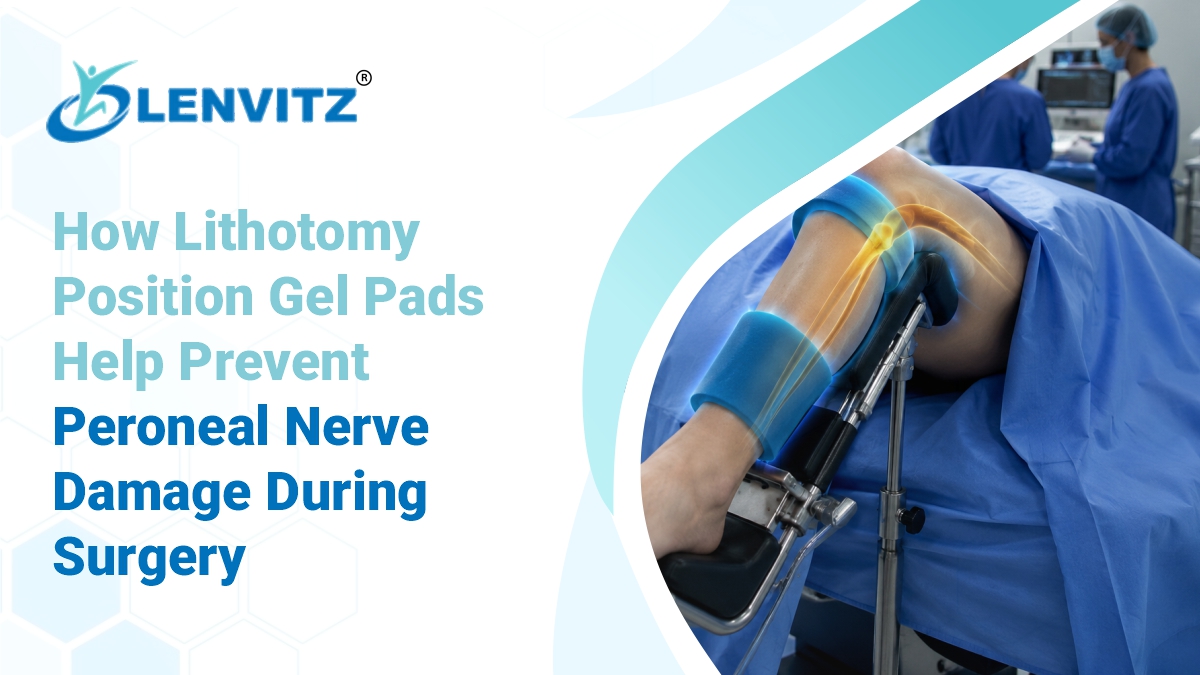
Lithotomy position gel pads are designed specifically to address this risk. By cushioning and stabilizing the lower limbs during procedures, they take pressure off the fibular head and protect the peroneal nerve through even long-duration surgeries.
What Is the Lithotomy Position and Where Is It Used
In the lithotomy position, the patient lies on their back with both legs raised, flexed at the hip and knee, and rested in stirrups. It provides surgeons with wide, unobstructed access to the perineum, pelvic floor, and lower abdomen making it the standard position for a wide range of procedures.
Common surgical specialties that use lithotomy positioning include:
- Gynaecological surgery — hysterectomies, laparoscopies, pelvic floor repairs
- Urological surgery — cystoscopies, prostatectomies, bladder procedures
- Colorectal surgery — rectal resections, haemorrhoidectomies, colposcopies
- Endoscopic procedures — colonoscopies and diagnostic lower GI scopes
- Obstetric and reproductive procedures
Because the limbs are held in a fixed, elevated position for the duration of the procedure, and because stirrups apply point pressure at specific contact zones, the risks associated with lithotomy positioning are distinct from those in supine, prone, or lateral surgical positions.
Why the Peroneal Nerve Is Particularly Vulnerable in Lithotomy Surgery
The common peroneal nerve, also known as the common fibular nerve, branches off the sciatic nerve and wraps around the head of the fibula, the bony prominence on the outer side of the knee. At this point, the nerve lies very close to the skin surface, with minimal soft tissue covering it.
This anatomical reality makes it highly susceptible to compression in any procedure where the lateral knee area rests against a hard surface or stirrup edge for an extended period. In lithotomy positioning, that risk is built into the position itself.
Several factors increase the likelihood of peroneal nerve injury during lithotomy procedures:
- Procedure duration: Risk rises significantly in surgeries lasting more than two hours, as sustained pressure has more time to disrupt blood supply and nerve function.
- Stirrup type and design: Poorly padded or rigid stirrups concentrate pressure directly on the fibular head.
- Patient build: Slender patients have less subcutaneous tissue over the nerve, reducing natural protection.
- Peripheral vascular disease: Reduced circulation to the nerve makes it more vulnerable to ischaemic injury from even moderate pressure.
- Incorrect leg height or angle: Positioning the legs too high or at an awkward angle increases lateral strain at the knee.
- Repeated repositioning: Adjustments during the procedure can introduce fresh friction and pressure at an already-compromised site.
What Peroneal Nerve Damage Looks Like After Surgery
Peroneal nerve injury often does not present immediately in recovery. Symptoms can emerge hours or days after the procedure, once the effects of anaesthesia wear off and the patient attempts normal movement.
Common signs include:
- Foot drop — an inability to lift the front of the foot, causing a distinctive dragging gait
- Numbness or reduced sensation along the outer lower leg and the top of the foot
- Weakness in ankle dorsiflexion and toe extension
- Tingling or burning along the lateral leg or dorsum of the foot
- Difficulty walking, climbing stairs, or bearing weight normally
Mild cases may resolve within weeks with physiotherapy and monitoring. Severe cases can result in permanent motor and sensory deficits, significantly affecting a patient’s quality of life and requiring long-term rehabilitation. The preventability of this injury is precisely why the choice of positioning support matters so much.
How Lithotomy Position Gel Pads Protect the Peroneal Nerve
Lithotomy position gel pads are placed at the knee and lower leg contact zones to cushion the fibular head and distribute leg weight across a broader surface. The goal is to eliminate concentrated pressure at the precise anatomical site where the common peroneal nerve is most exposed.
Cushioning the fibular head directly
Medical-grade silicone gel conforms to the contour of the outer knee, filling the gap between the leg and the stirrup surface. This removes the hard point contact at the fibular head that is the primary mechanical cause of peroneal nerve compression.
Reducing sustained pressure throughout the procedure
Silicone gel pads maintain their cushioning properties under load, unlike foam which can compress and lose its protective depth within the first hour of a procedure. For long lithotomy surgeries, this sustained pressure relief is critical, the pad continues to protect the nerve at the two-hour mark just as effectively as at the start.
Maintaining consistent limb alignment
Lithotomy position gel pads stabilize the leg within the stirrup, reducing micro-movements that can shift the nerve against a hard edge during the procedure. Consistent alignment also prevents the leg from rotating inward, which can increase torsional strain on the peroneal nerve at the fibular head.
Supporting the full limb, not just the knee
Well-designed lithotomy gel pads support the calf and lower leg in addition to the knee, distributing the weight of the raised limb more evenly. Some setups also incorporate supine position gel pads at the heel and sacrum to address pressure across the entire lower body during combined supine-lithotomy positioning, which is common in many urological and gynaecological procedures.
Other Nerve and Pressure Risks in Lithotomy Positioning
The peroneal nerve is the most commonly injured, but it is not the only structure at risk in lithotomy surgery. Positioning teams should account for the full range of pressure and stretch risks this position creates.
- Sciatic nerve: Excessive hip flexion or external rotation can stretch or compress the sciatic nerve, particularly in patients with limited hip mobility.
- Femoral nerve: Over-flexion at the hip combined with abduction can stretch the femoral nerve, causing thigh weakness or sensory changes postoperatively.
- Obturator nerve: Extreme abduction places the obturator nerve under traction, a risk that increases with more aggressive leg positioning.
- Sacral pressure injuries: In the supine component of lithotomy positioning, the sacrum and coccyx bear significant load. Supine position gel pads at these bony prominences reduce the risk of deep tissue pressure injuries during extended procedures.
- Compartment syndrome: Prolonged elevated leg positioning can impair venous return, causing calf compartment pressure to rise a serious, time-sensitive complication in very long lithotomy cases.
For a detailed look at how nerve injuries occur in other surgical positions, including lateral procedures where the brachial plexus and ulnar nerve are at risk, see our guide to lateral position gel pads and nerve protection in the OT.
The Role of Supine Position Gel Pads in Lithotomy Procedures
Most lithotomy procedures begin with the patient in a flat supine position before the legs are elevated into stirrups. During this phase and in the back and torso throughout the entire procedure, the pressures of the supine position still apply.
Supine position gel pads placed at the sacrum, coccyx, and heels provide continuous pressure relief across the posterior body for the duration of the procedure. These pads work alongside lithotomy-specific knee and leg pads, addressing the full map of pressure points rather than just the lower limbs.
For facilities performing frequent lithotomy or combined supine-lithotomy procedures, a paired approach dedicated lithotomy position gel pads at the knee and calf, supine position gel pads at the sacrum and heels gives the most comprehensive protection across the patient’s posterior surface.
Lithotomy Positioning vs Lateral Positioning — Different Risks, Different Support
Understanding the difference between lithotomy and lateral positioning is important for choosing the right gel pad configuration. While both carry nerve injury risks, the mechanisms and vulnerable anatomy differ significantly.
In lithotomy surgery, the patient lies supine with legs elevated. The primary risk is compression at the fibular head from stirrup contact. The peroneal nerve, sciatic nerve, and femoral nerve are the main structures at risk, and lithotomy position gel pads address these by cushioning the knee and calf contact zones.
In lateral surgery, the patient lies on one side. A lateral positioner is used to stabilize the torso and pelvis in position, preventing the patient from rolling forward or back during the procedure. The primary nerve risk in this position is the brachial plexus and ulnar nerve, with additional pressure risks at the hips, shoulders, and lateral knee. Lateral position gel pads protect these zones and keep the body safely aligned throughout procedures like thoracic, orthopedic, and renal surgery.
Facilities that perform both lithotomy and lateral procedures should maintain gel pad sets suited to each positioning type, as the anatomical contact zones and the pressures at risk are quite different.
Choosing the Right Lithotomy Position Gel Pads for Your OT
Selecting appropriate gel pads for lithotomy procedures involves matching the pad specification to the clinical context. Browse Lenvitz’s full range of patient positioning gel pads for specifications, or use the criteria below to guide your selection.
Target the fibular head specifically
Look for pads designed with a contoured recess or raised perimeter that offloads the fibular head while still supporting the surrounding calf tissue. Generic pads that apply uniform contact across the knee may still create concentrated pressure at this point.
Confirm sustained performance under load
Medical-grade silicone gel maintains its pressure-redistribution properties through multi-hour procedures. Confirm that the pad material holds its shape and cushioning depth under sustained weight before using it in long-duration surgeries.
Pair with compatible stirrup systems
Gel pads should fit the stirrup type used in your facility — whether candy cane stirrups, boot-style supports, or Allen-type leg holders. A pad that slips or bunches within the stirrup introduces positioning instability and the very pressure points it was designed to prevent.
Consider the full lower-body setup
Plan for heel and sacral support as well as knee and calf protection. A complete lithotomy positioning setup that includes supine position gel pads at the posterior contact zones gives the broadest protection across the procedure.
Factor in procedure duration and patient profile
Elderly patients, those with peripheral vascular disease, or bariatric patients in long procedures have elevated risk profiles that justify more comprehensive padding. Thinner patients need extra attention at the fibular head due to reduced subcutaneous protection over the nerve.
Best Practices for Peroneal Nerve Protection in Lithotomy Positioning
Conduct a preoperative nerve injury risk assessment
Before positioning, note any existing peripheral neuropathy, vascular disease, prior nerve injuries, BMI, and estimated procedure duration. Higher-risk patients warrant additional padding and more frequent intraoperative checks.
Apply lithotomy position gel pads before the patient is placed in stirrups
Position the pads in the stirrups before the legs are lifted, rather than attempting to insert them after the patient is already in position. This ensures the pad is correctly placed at the fibular head contact zone from the start.
Check alignment of both legs symmetrically
Asymmetric positioning, where one leg is angled differently from the other, concentrates pressure unevenly and increases nerve risk on the more compressed side. Confirm that both legs are at the same height and angle before the procedure begins.
Monitor positioning at regular intervals during long procedures
For procedures expected to run beyond 90 minutes, recheck the gel pad position and look for any migration away from the fibular head. Brief intraoperative checks can catch a shifted pad before it becomes a nerve injury.
Lower both legs simultaneously at the conclusion of the procedure
Lowering legs one at a time after a long lithotomy procedure can cause sudden haemodynamic shifts and uneven reperfusion. Lower both legs slowly and together, and monitor the patient closely in the immediate post-procedure period.
Document positioning and pad placement in the surgical record
Record which pads were used, where they were placed, how long the patient was in lithotomy position, and the result of any intraoperative positioning checks. This documentation supports postoperative assessment if nerve symptoms arise.
Conclusion
Peroneal nerve injury in lithotomy surgery is preventable. The anatomy is well understood, the risk factors are identifiable, and the protective measure is straightforward: the right lithotomy position gel pads, correctly placed and paired with consistent intraoperative monitoring.
By cushioning the fibular head, redistributing limb weight, and maintaining stable alignment throughout the procedure, silicone gel pads remove the mechanical pressure that is the primary driver of peroneal nerve damage in the OT. Combined with supine position gel pads at the sacrum and heels, and supported by a disciplined positioning protocol, they give surgical teams a reliable way to protect patients through even the longest lithotomy procedures.
As with lateral positioning where a lateral positioner and lateral position gel pads address the distinct nerve risks of side-lying surgery, the key is matching the right support to the right position. Lithotomy has its own risk profile, and its own solution.
FAQ’s
The common peroneal nerve wraps around the head of the fibula (the lateral bony prominence at the outer knee) with very little protective tissue over it. In lithotomy positioning, the leg rests against the stirrup at this exact point. Sustained pressure at the fibular head over the course of a long procedure can compress the nerve, disrupt blood supply, and cause varying degrees of nerve injury.
They cushion the fibular head contact zone with medical-grade silicone gel that conforms to the outer knee and distributes leg weight across a wider surface. This removes the concentrated mechanical pressure on the nerve that causes injury, and unlike foam, silicone maintains its protective depth throughout the full duration of the procedure.
Lithotomy position gel pads target the knee and calf contact zones in the stirrups, protecting the peroneal nerve at the fibular head. Supine position gel pads address the posterior body sacrum, coccyx, and heels which remain in contact with the OT table throughout a lithotomy procedure. Both are typically needed for complete lower-body protection.
Lithotomy positioning places the patient supine with legs elevated in stirrups, creating nerve risk primarily at the fibular head, sciatic, and femoral nerve territories. Lateral positioning places the patient on their side, requiring a lateral positioner for torso stability and lateral position gel pads at the hips, shoulders, knees, and lateral head to protect the brachial plexus, ulnar nerve, and peroneal nerve. The contact zones and the anatomy at risk are different, so the pad configuration differs significantly between the two.