Nerve injuries are among the most feared and least discussed complications of surgical positioning. A patient enters the operating theatre for a kidney resection, a thoracic procedure, or a hip replacement and leaves with pain, numbness, or weakness that has nothing to do with the surgery itself. Position-related peripheral nerve injuries are estimated to account for 16% of all anaesthesia-related claims in surgical settings globally, and the lateral decubitus position is one of the highest-risk configurations for exactly this type of complication.
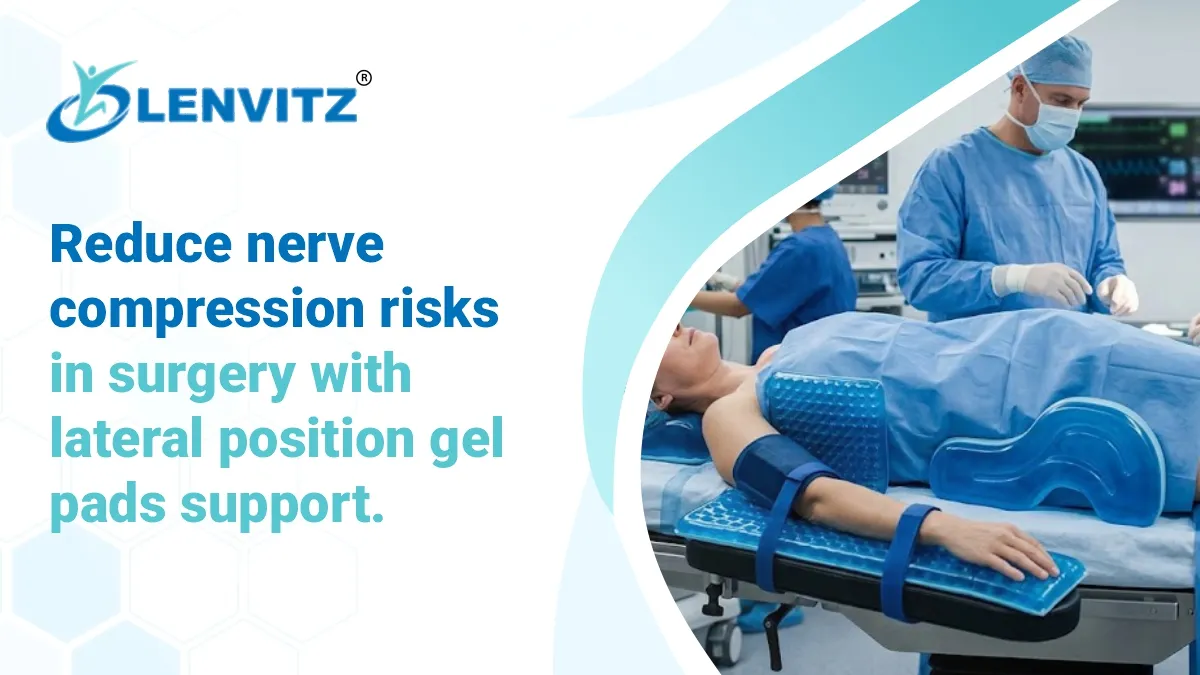
The lateral decubitus position places the patient on their side, with the dependent arm, shoulder, axilla, and lower extremities all under sustained compressive and tensile stress for the duration of the procedure. Without correctly designed lateral position gel pads supported beneath and around the body, the pressure concentrations and stretch forces on peripheral nerves, the brachial plexus, common peroneal nerve, and ulnar nerve in particular are clinically significant even in procedures under 90 minutes.
A lateral positioner built from medical-grade silicon gel pads is not merely a comfort accessory. It is a patient safety device that directly determines whether the surgical team controls the forces acting on the patient’s nerves or leaves them entirely to chance.
Why the Lateral Decubitus Position Creates Unique Nerve Compression Risk
To understand why lateral position gel pads support matters so much, it helps to understand what the lateral position actually does to the body. Unlike the supine position, where weight is distributed relatively symmetrically across the posterior surface, the lateral decubitus position creates highly asymmetric loading across the body. The dependent side bears the full weight of the torso, shoulder girdle, hip, and lower leg in a configuration that concentrates compressive force on a narrow band of bony prominences. The non-dependent side is simultaneously held in an elevated, often unsupported position that places the peripheral nerves under traction.
The key nerve injury mechanisms in the lateral position:
- Brachial plexus compression – The dependent shoulder is forced upward and inward if unsupported, creating a stretch-compression injury to the brachial plexus roots between the clavicle and first rib. This is the most common serious nerve injury in lateral positioning and produces symptoms ranging from transient paraesthesia to permanent upper limb weakness
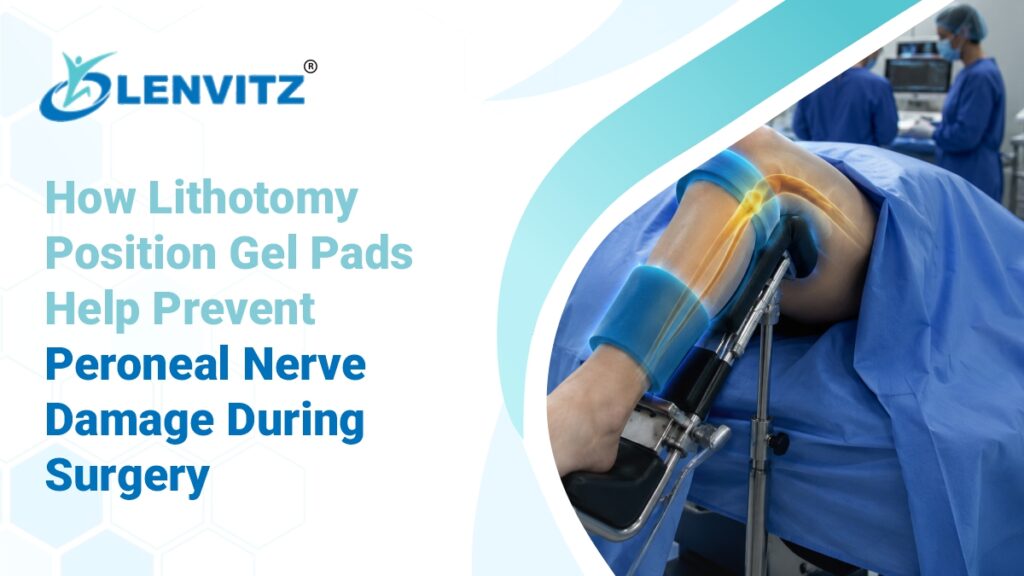
- Common peroneal nerve compression – The fibular head of the dependent leg rests directly on the table surface without padding, compressing the common peroneal nerve as it wraps around the proximal fibula. Even moderate pressure sustained for 30 minutes can cause foot drop that may take months to resolve
- Ulnar nerve compression – The medial epicondyle of the dependent elbow contacts the table surface when the arm is left in an unsupported position, producing the classic sensory loss across the ring and little finger
- Femoral nerve traction – Excessive hip flexion on the non-dependent side places the femoral nerve under stretch, a risk that increases with steep table angulation and prolonged procedure time
- Axillary neurovascular compression – Without an axillary roll or correctly positioned gel pads support beneath the dependent chest wall, the axillary vessels and nerves are compressed by the weight of the entire upper torso
Understanding how silicon gel pads prevent pressure ulcers and nerve injuries in surgical positioning is the first step toward an evidence-based lateral positioning protocol.
What Lateral Position Gel Pads Actually Do
The mechanical function of lateral position gel pads encompasses three distinct protective mechanisms that go beyond simple cushioning.
1. Pressure Redistribution Across Bony Prominences
Medical-grade silicon gel pads are viscoelastic, they flow and conform under load, redistributing compressive force away from bony prominences across a wider soft tissue surface area. The fibular head does not create a point pressure concentration when resting on a conforming gel pad; instead, the contact area increases and peak interface pressure drops below the threshold for sustained ischaemic nerve injury.
2. Positional Stability That Prevents Nerve Traction
A correctly configured lateral positioner system stabilises the patient in the intended position throughout the procedure, preventing the progressive position drift that occurs when patients are placed on hard surfaces or inadequate padding. A patient who starts in a well-aligned lateral position but drifts 15 degrees posteriorly over two hours is accumulating brachial plexus traction injury the entire time without any single obvious moment of misalignment.
3. Cushioning of the Axillary Space and Dependent Shoulder
The dependent shoulder and axilla are the anatomical zone most consistently associated with serious lateral positioning nerve injuries. A correctly placed axillary gel pad or chest roll creates a supported gap that lifts the chest wall away from the table surface, decompressing the axillary neurovascular bundle and reducing the upward displacement force on the brachial plexus.
For the full clinical picture of how gel pads function as surgical positioning devices, see gel pads used as surgical positioning devices in the lithotomy position.
The Lateral Decubitus Position Across Surgical Specialties
1. Thoracic Surgery
Thoracic procedures, lobectomies, thoracoscopic lung resections, oesophageal procedures are performed in the lateral decubitus position almost universally. These are among the longest lateral position cases in routine surgical practice, with procedure times routinely exceeding 3–4 hours. Every element of the positioning protocol is therefore under maximum stress.
Primary nerve compression risks in thoracic lateral positioning:
- Brachial plexus injury from dependent shoulder upward displacement without axillary support
- Ulnar nerve compression at the medial epicondyle of the dependent arm
- Common peroneal nerve injury at the fibular head of the dependent leg
- Contralateral femoral nerve traction if hip flexion is excessive
Key benefits of silicon gel pads support in thoracic positioning:
- Axillary roll support using a longitudinal gel pad beneath the dependent chest wall, placed distal to the axilla, lifts the thorax and directly reduces brachial plexus compression
- Between-the-knees gel pads prevent adduction and internal rotation of the dependent leg, protecting the common peroneal nerve
- Dependent arm board with silicon gel pads padding maintains the arm in a neutral position without contact pressure at the medial epicondyle
- Full-body lateral positioner systems stabilise the patient against the torque forces of the open thoracic cavity without rigid strapping that creates its own pressure points
2. Urological Surgery
Nephrectomy, partial nephrectomy, pyeloplasty, and adrenalectomy are all performed in modified lateral or flank positions. The flank position introduces additional risk because the patient is often kidney-elevated with the table flexed, creating a lateral bowing of the torso that stretches the dependent lateral structures while simultaneously elevating the contralateral flank.
Key nerve risks in urological lateral positioning:
- Lateral femoral cutaneous nerve compression at the iliac crest of the dependent hip producing meralgia paraesthetica post-operatively
- Dependent leg peroneal nerve compression amplified by table flexion increasing pressure on the fibular head
- Brachial plexus traction on the non-dependent side if the arm is not adequately supported above the torso
A Wedge Lateral Positioner with medical-grade silicon gel pads surface provides the conforming, pressure-distributing support that standard foam wedges cannot match across a 3–4 hour urological procedure. Explore the full lateral positioner product range including the Lateral Gel Positioning Bed and Lateral Leg Positioner – Foam with Gel Top for urological applications.
3. Orthopaedic Surgery
Total hip arthroplasty performed in the lateral position, hip arthroscopy, and certain femoral procedures require precise lateral positioning. Orthopaedic procedures involve significant physical forces retraction, reaming, hammering that are transmitted through the positioning system to the patient’s contact surfaces.
Key positioning challenges in orthopaedic lateral cases:
- Surgical forces create movement that standard foam positioners cannot resist, increasing drift-related traction risk
- Dependent greater trochanter pressure is a documented source of lateral cutaneous nerve injury
- The non-operative limb must be supported in a position that does not create traction on the sciatic or femoral nerve
Why silicon gel pads outperform foam in orthopaedic lateral cases:
Standard foam positioners compress and deform under the repeated physical loads of orthopaedic procedures. Once a foam wedge bottoms out, the patient is effectively resting on the table surface through the collapsed padding. Medical-grade silicon gel pads maintain their pressure-distributing properties under sustained and dynamic mechanical load, ensuring continuous nerve protection throughout procedures that combine long duration with high physical forces.
4. Neurosurgery and Spine Surgery
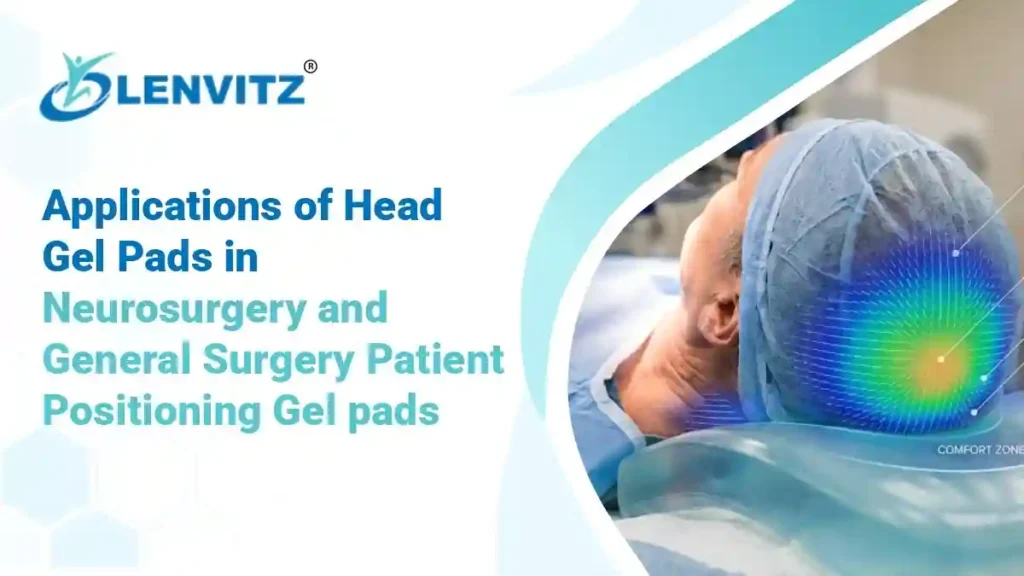
Lateral approach spinal procedures far lateral lumbar interbody fusion (XLIF/LLIF), lateral thoracic discectomy, and certain craniotomies require the precision lateral positioning and nerve protection demands of both neurosurgery and spine surgery simultaneously. The principles of head and body positioning for lateral approach spine surgery are closely related to those covered in applications of head gel pads in neurosurgery and general surgery patient positioning, with the additional requirement that lumbar spine alignment in the lateral position is precisely controlled by the lateral positioner configuration.
Choosing the Right Lateral Position Gel Pads: Quick Reference
| Surgical Specialty | Recommended Lateral Positioner | Primary Nerve Protected |
|---|---|---|
| Thoracic Surgery | Lateral Gel Positioning Bed + axillary gel pad | Brachial plexus, ulnar nerve |
| Nephrectomy / Flank | Wedge Lateral Positioner with silicon gel pads | Peroneal, lateral femoral cutaneous |
| Total Hip Arthroplasty | Full lateral positioner with between-leg gel pads | Sciatic, peroneal, femoral |
| Lateral Spine / XLIF | Precision lateral positioner with thoracic & pelvic support | Lumbar plexus, femoral nerve |
| Paediatric Lateral Cases | Paediatric silicon gel pads scaled positioners | All peripheral nerves |
A Positioning Protocol Checklist for the OT Team
Before committing the patient to the lateral decubitus position, the scrub nurse, anaesthetist, and surgeon should collectively confirm:
- The dependent shoulder is not bearing the full torso weight, an axillary gel pad or chest roll is correctly placed distal to the axilla, not under it
- The dependent arm is positioned on a padded arm board with no contact pressure at the medial epicondyle
- A between-the-knees silicon gel pad or pillow is in place, preventing adduction of the dependent leg and protecting the fibular head
- The dependent leg is straight or slightly flexed, not sharply flexed at the knee, which would increase peroneal nerve tension
- The lateral positioner is stabilising the pelvis and thorax without rigid straps that create their own focal pressure points
- All bony prominences fibular head, iliac crest, greater trochanter, medial epicondyle, lateral malleolus have been checked for adequate padding before drapes are applied
- Position is re-verified after final draping and before incision, particularly if anaesthetic induction required any significant patient movement
- For procedures over 2 hours, intra-operative position check is built into the team’s protocol
The broader principles of how silicon gel pads prevent pressure ulcers in surgical settings apply fully to nerve compression prevention in lateral positioning.
The Indian OT Context
Nerve compression injuries from lateral positioning are underreported in Indian surgical settings, not because they occur less frequently but because the connection between the positioning protocol and the post-operative neurological complaint is often not made. A patient who reports hand weakness or foot drop after a nephrectomy is frequently investigated for surgical causes before positioning-related injury is considered.
Indian teaching hospitals with high surgical volumes perform large numbers of thoracic, urological, and orthopaedic lateral position cases daily. The standard positioning equipment in many of these theatres remains basic foam wedges and rolled blankets materials that lack the conforming, sustained pressure redistribution properties of medical-grade lateral position gel pads.
The investment in certified silicon gel pads-based lateral positioner systems is not a luxury upgrade for premium private hospitals. It is a clinical standard that directly reduces medico-legal risk, improves patient outcomes, and aligns Indian OT practice with NABH and international positioning guidelines.
FAQ’s
The threshold varies by nerve and individual patient factors. Sustained interface pressure above 30–32 mmHg for more than 2 hours is the widely cited threshold for ischaemic nerve injury. However, for highly vulnerable sites like the common peroneal nerve at the fibular head, clinically significant injury has been documented in procedures as short as 45–60 minutes without adequate gel pads protection.
Yes, for sustained procedures. Foam provides initial cushioning but progressively bottoms out under sustained load, meaning effective protection degrades over the course of the procedure. Medical-grade silicon gel pads maintain their viscoelastic properties throughout, providing consistent pressure redistribution from incision to closure. This is especially critical for lateral cases which typically run 2–5 hours.
Correct axillary support. The axillary gel pad or chest roll placed beneath the dependent chest wall, distal to the axilla, is the single most protective step for the brachial plexus. Without it, the full weight of the upper thorax drives the shoulder into the neck, compressing the plexus between the clavicle and first rib for the entire procedure.
For procedures exceeding 3 hours, an intra-operative position check is recommended. The team should confirm that no drift has occurred, that padding remains in correct position, and that no new pressure points have developed. Silicon gel pads positioners are more resistant to position drift than foam but should still be verified during extended cases.